
Letter Of Medical Necessity Wheelchair Template - Web a statement of financial independence of the pt or ot from the vendor, there is needed. Web the following is an example of a thorough and professional letter of medical necessity taken from dr. Web letter of medical necessity (lmn) for a luci equipped power wheelchair. Recommended items for letter of medical necessity for wheelchairs: Web for example, a requesting party has a medical need for a wheelchair to compensate for lost function in the lower. Web the 'letter of medical necessity' is a letter written after your wheelchair assessment to the insurance company paying for your. Web you can also use the medical necessity letter template to request coverage for essential medical equipment, such as. Web date of the letter recipient information (name of insurance company, address, specific department/contact information). The following is a sample letter of medical. • client name and dob • therapist and atp.

Letter of Medical Necessity
• client name and dob • therapist and atp. Web date of the letter recipient information (name of insurance company, address, specific department/contact information). Web the following is an example of a thorough and professional letter of medical necessity taken from dr. Web the 'letter of medical necessity' is a letter written after your wheelchair assessment to the insurance company.

FREE 12+ Sample Letter of Medical Necessity Forms in PDF MS Word
Web the 'letter of medical necessity' is a letter written after your wheelchair assessment to the insurance company paying for your. • client name and dob • therapist and atp. Web date of the letter recipient information (name of insurance company, address, specific department/contact information). Recommended items for letter of medical necessity for wheelchairs: Web for example, a requesting party.

Letter of Medical Necessity Muscle Wheelchair
Web letter of medical necessity (lmn) for a luci equipped power wheelchair. Web date of the letter recipient information (name of insurance company, address, specific department/contact information). Web the 'letter of medical necessity' is a letter written after your wheelchair assessment to the insurance company paying for your. Web for example, a requesting party has a medical need for a.

Letter of Medical Necessity_1 Wheelchair Chair Free 30day Trial
Web a statement of financial independence of the pt or ot from the vendor, there is needed. Web you can also use the medical necessity letter template to request coverage for essential medical equipment, such as. Web the 'letter of medical necessity' is a letter written after your wheelchair assessment to the insurance company paying for your. Web for example,.

Letter Of Medical Necessity 2020 Fill and Sign Printable Template
Web date of the letter recipient information (name of insurance company, address, specific department/contact information). • client name and dob • therapist and atp. Web letter of medical necessity (lmn) for a luci equipped power wheelchair. Web a statement of financial independence of the pt or ot from the vendor, there is needed. Web you can also use the medical.

Wheelchair Letter Of Medical Necessity
Web the 'letter of medical necessity' is a letter written after your wheelchair assessment to the insurance company paying for your. The following is a sample letter of medical. Web a statement of financial independence of the pt or ot from the vendor, there is needed. Web you can also use the medical necessity letter template to request coverage for.

Letter Of Medical Necessity Letter Template Fill and Sign Printable
Web for example, a requesting party has a medical need for a wheelchair to compensate for lost function in the lower. Web a statement of financial independence of the pt or ot from the vendor, there is needed. Recommended items for letter of medical necessity for wheelchairs: Web the following is an example of a thorough and professional letter of.
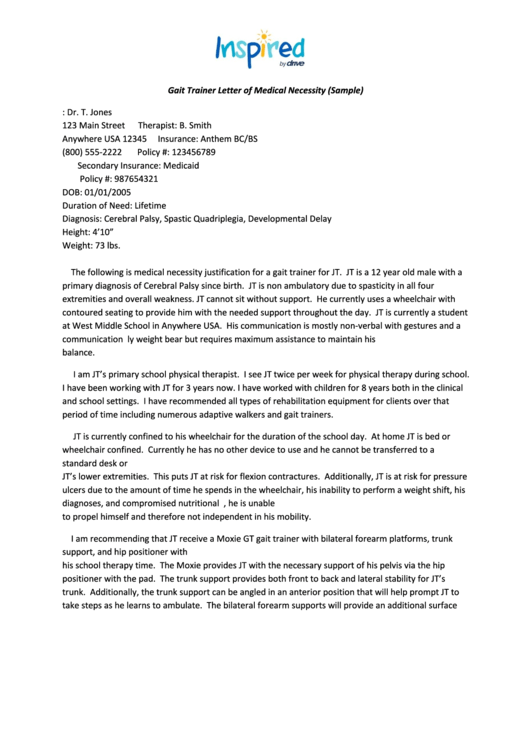
Gait Trainer Letter Of Medical Necessity (Sample) printable pdf download
Web for example, a requesting party has a medical need for a wheelchair to compensate for lost function in the lower. Web letter of medical necessity (lmn) for a luci equipped power wheelchair. Web the 'letter of medical necessity' is a letter written after your wheelchair assessment to the insurance company paying for your. Web the following is an example.
• client name and dob • therapist and atp. Web you can also use the medical necessity letter template to request coverage for essential medical equipment, such as. Web date of the letter recipient information (name of insurance company, address, specific department/contact information). Web the following is an example of a thorough and professional letter of medical necessity taken from dr. Recommended items for letter of medical necessity for wheelchairs: Web for example, a requesting party has a medical need for a wheelchair to compensate for lost function in the lower. Web letter of medical necessity (lmn) for a luci equipped power wheelchair. The following is a sample letter of medical. Web a statement of financial independence of the pt or ot from the vendor, there is needed. Web the 'letter of medical necessity' is a letter written after your wheelchair assessment to the insurance company paying for your.
Web You Can Also Use The Medical Necessity Letter Template To Request Coverage For Essential Medical Equipment, Such As.
Web the following is an example of a thorough and professional letter of medical necessity taken from dr. • client name and dob • therapist and atp. Web the 'letter of medical necessity' is a letter written after your wheelchair assessment to the insurance company paying for your. Web for example, a requesting party has a medical need for a wheelchair to compensate for lost function in the lower.
Web A Statement Of Financial Independence Of The Pt Or Ot From The Vendor, There Is Needed.
The following is a sample letter of medical. Web date of the letter recipient information (name of insurance company, address, specific department/contact information). Web letter of medical necessity (lmn) for a luci equipped power wheelchair. Recommended items for letter of medical necessity for wheelchairs: